Chest X-Ray for the Internist
Question 1Posted on: Jan 10th 2020
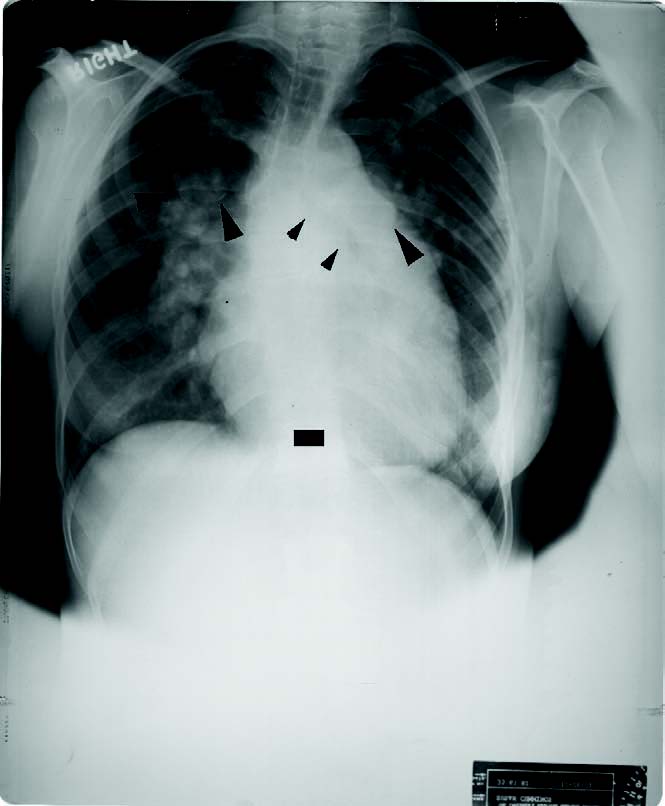
This PA radiograph of a 24-year-old woman shows
(Courtesy Amgad N. Makaryus, MD @AmgadMakaryus Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Pulmonary Stenosis
- Pulmonary Hypertension
- Hilar Adenopathy
- Systemic Hypertension
Show Answer
Answer: Choice 2: Pulmonary Hypertension
Explanation:
This is PA radiograph of a 24-year-old woman with a ventricular septal defect and two-thirds systemic pulmonary hypertension. Kyphoscoliosis displaces the chest toward the left. Thin curvilinear calcification of dilated central pulmonary artery segments (large arrowheads) are found bilaterally. Notice the increased caliber of the right hilar pulmonary artery and how the rotated left heart border appears to lie parallel to the left bronchus (small arrowheads).
Pulmonary artery calcification is unusual and nearly always associated with a dilated PA segment and bilateral dilated hilar PAs and pulmonary hypertension (Figure). Increased pulmonary artery pressure, increased flow, and the combination of increased pressure and flow all cause dilatation of the PA segment. Furthermore, these conditions are all associated with increased caliber of the hilar PAs, as well.
Bilateral hilar adenopathy most commonly mimics dilated pulmonary arteries, but is not commonly associated with a dilated main PA segment.
Increased PA pressure is the result of the response of the right ventricle to the elevation of pulmonary vascular resistance, which is controlled by the post hilar pulmonary bed. Thus, on radiographs of patients with pulmonary hypertension of any etiology, one expects to see the combination of dilatation of the PA segment and hilar PAs, associated with vasoconstriction of the peripheral bed. This produces a dramatic change in vessel caliber between the central and peripheral pulmonary vasculature. As vessel caliber in the periphery decreases, the smaller vessels fall beneath the spatial resolution of the imaging system and seem to disappear. The lung fields appear darker (fewer visualized vessels) and vessels do not appear to extend as far to the lung periphery.
The radiographic differential diagnosis of pulmonary hypertension is organized around associated radiographic findings (i.e., hyperaeration or flat diaphragms in COPD; interstitial lung changes and bronchiectasis in cystic fibrosis; a normal left ventricle, with a dilated left atrium and interstitial change in mitral stenosis; right heart dilatation with a normal left heart in ASD).
The caliber of the PA segment itself does not correlate well with the severity of the pulmonary hypertension.
Question 2Posted on: Jan 13th 2019
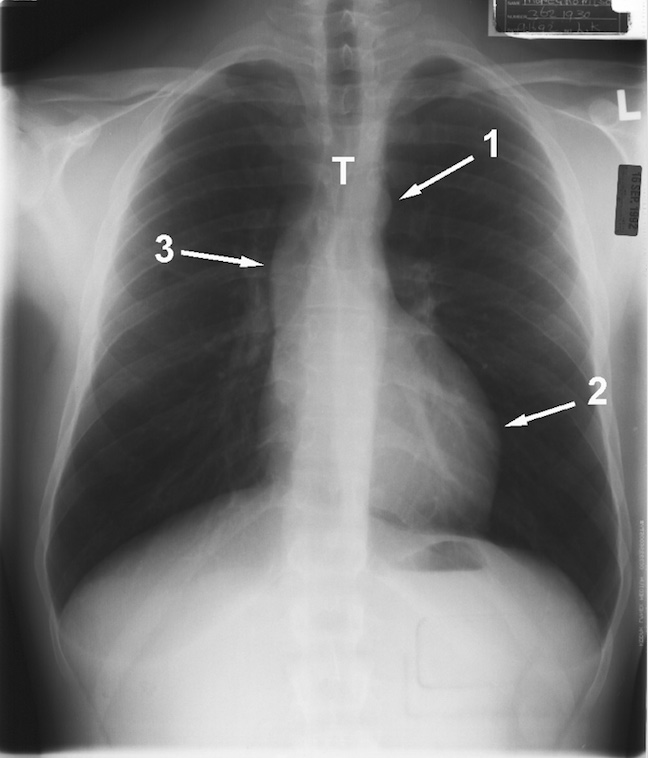
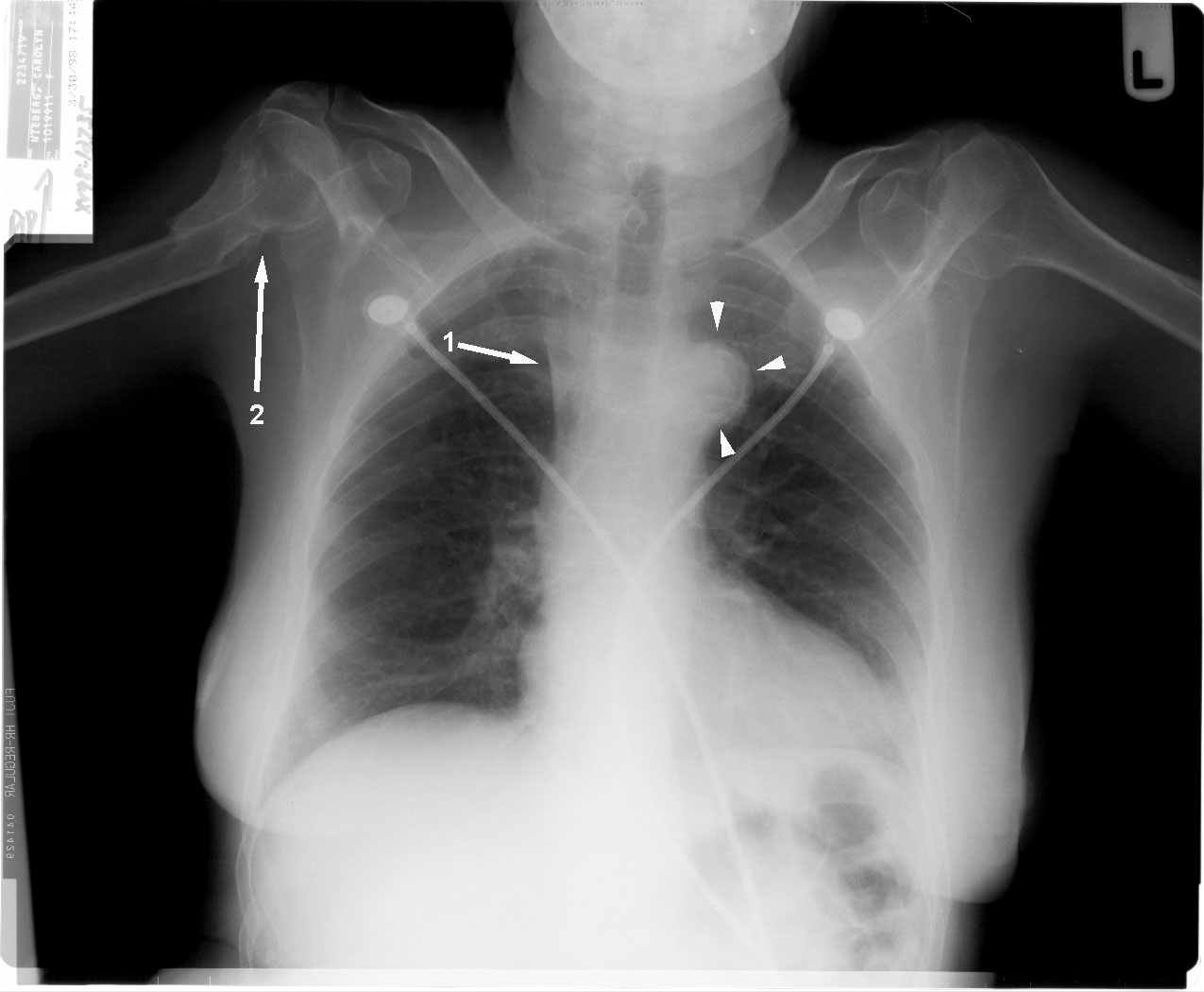
A 24-year old male has a chest x-ray. This radiograph suggests that patient has an (Courtesy Amgad N. Makaryus, MD @AmgadMakaryus Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Aortic aneurysm
- Aortic Dissection
- Aortic pseudoaneurysm
- Mass adjacent to the aortic arch
- Coarctation of the aorta
Show Answer
Answer: Choice 5: Coarctation of the Aorta
Explanation:
This patient has both coarctation of the aorta and bicuspid aortic valve stenosis. The aortic arch shadow (arrow 1) small, and barely displaces the trachea (T) to the right.
Also notice the rounded contour of the hypertrophied left ventricular segment (arrow 2),
And the extension of the ascending aortic shadow (arrow 3) over the right hilum, secondary to post stenotic dilatation.
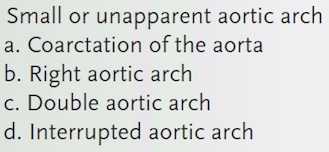
A small, or inconspicuous aortic arch segment is one that requires a second look to be sure that it is actually there (Figure).
If the trachea is not displaced toward the right, then (1) the aortic arch may be small, or (2), it may not be present.
The differential diagnosis of a small or unapparent aortic arch is given in Table: (Derived from • Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516)
Question 3Posted on: Jan 13th 2019
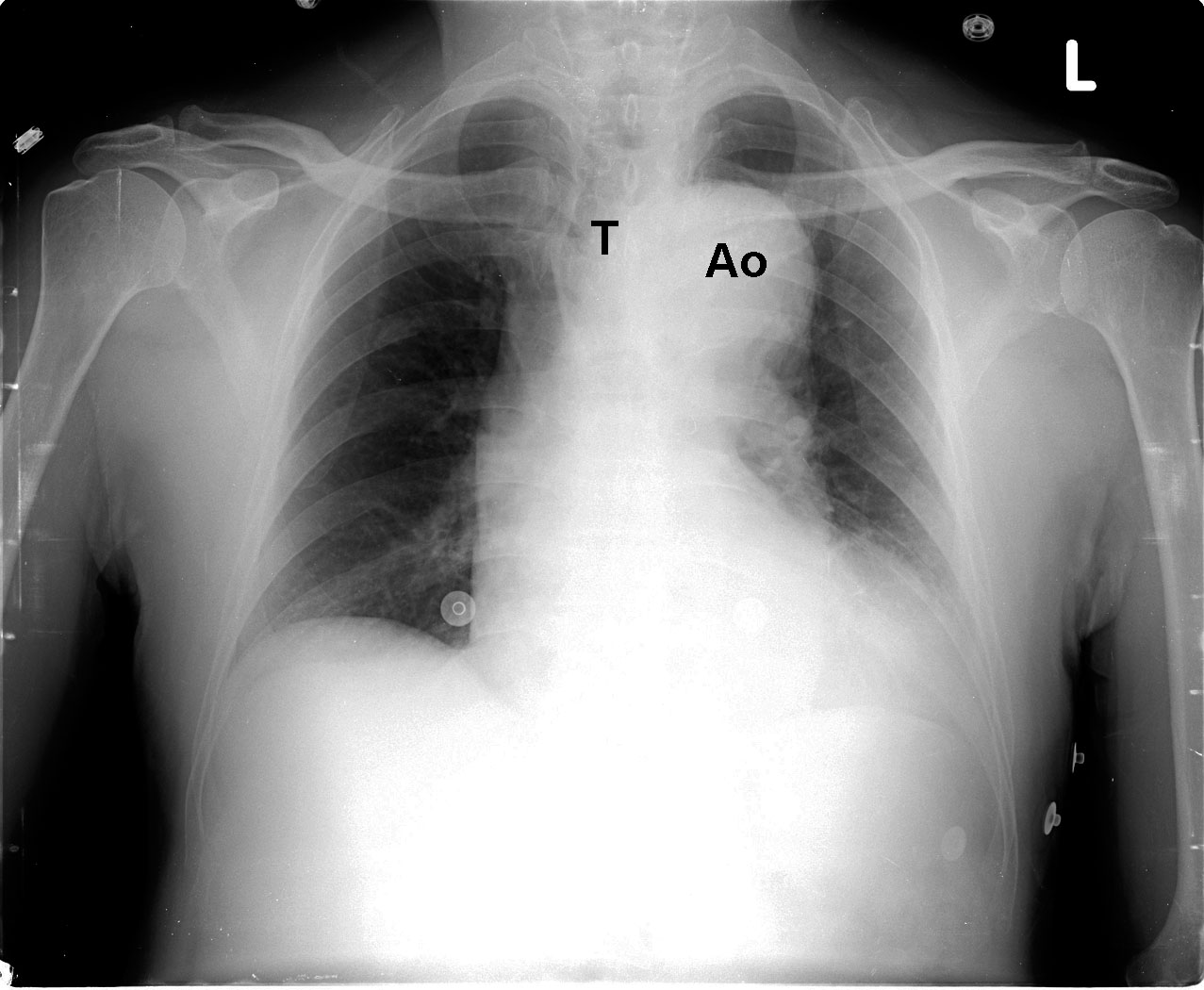
A 73-year old male complains of cough. This AP chest radiograph shows (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Right aortic arch
- Coarctation of aorta
- Double aortic arch
- Interrupted aortic arch
- Aortic aneursym
Show Answer
Answer: Choice 5: Aortic aneurysm
Explanation:
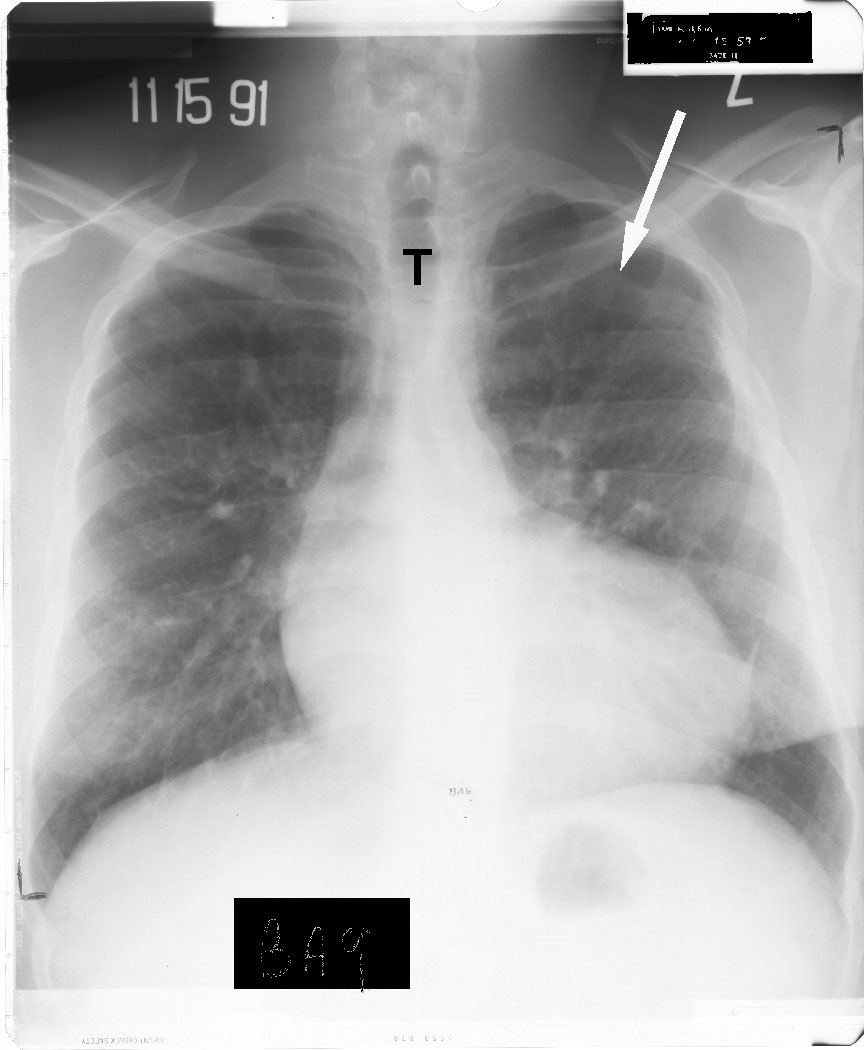
The aortic arch (Ao) is markedly enlarged (measuring 38 mm) representing an aneurysm
Notice the displacement of the tracheal air shadow (T) to the right, by the prominent extension into the transverse arch
Dilatation of the aortic arch is defined as the presence of an arch segment > 25 mm from trachea to the left hear border
Derived from • Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
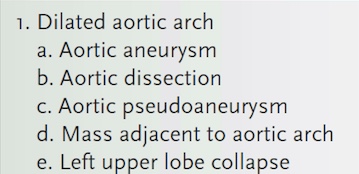
Differential Diagnosis of Aortic Arch includes:
Question 4Posted on: Jan 13th 2019
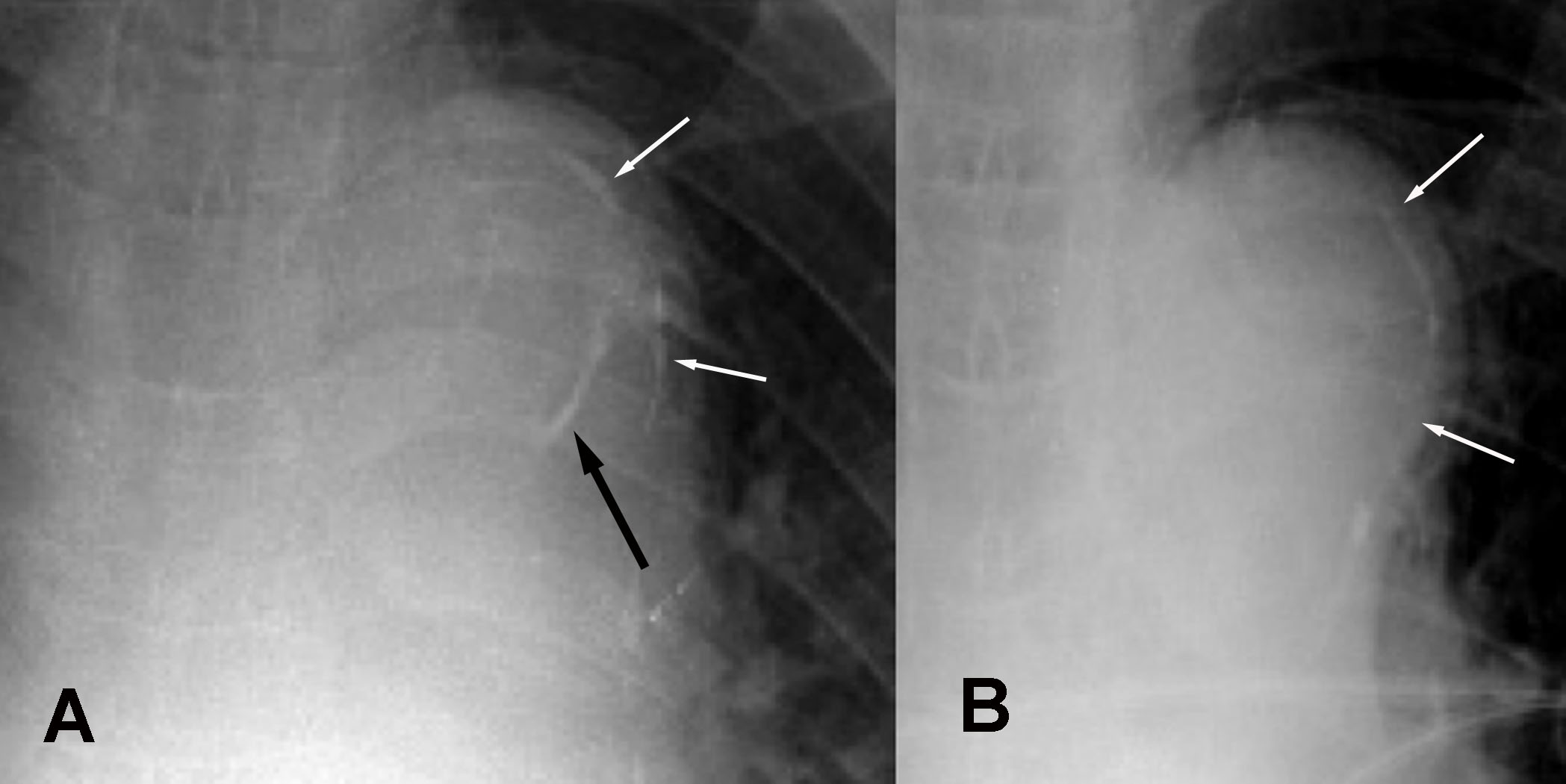
A 67-year old man complains of upper back pain. These cropped views from PA chest films where A) is admitting radiograph and B) is previous examination obtained 2 years prior to this examination. Radiograph A shows (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Acute aortic dissection
- Normal aorta
- Calcified aorta that is usually seen with aging
- Dilated trachea
Show Answer
Answer: Choice 1: Acute aortic dissection
Explanation:
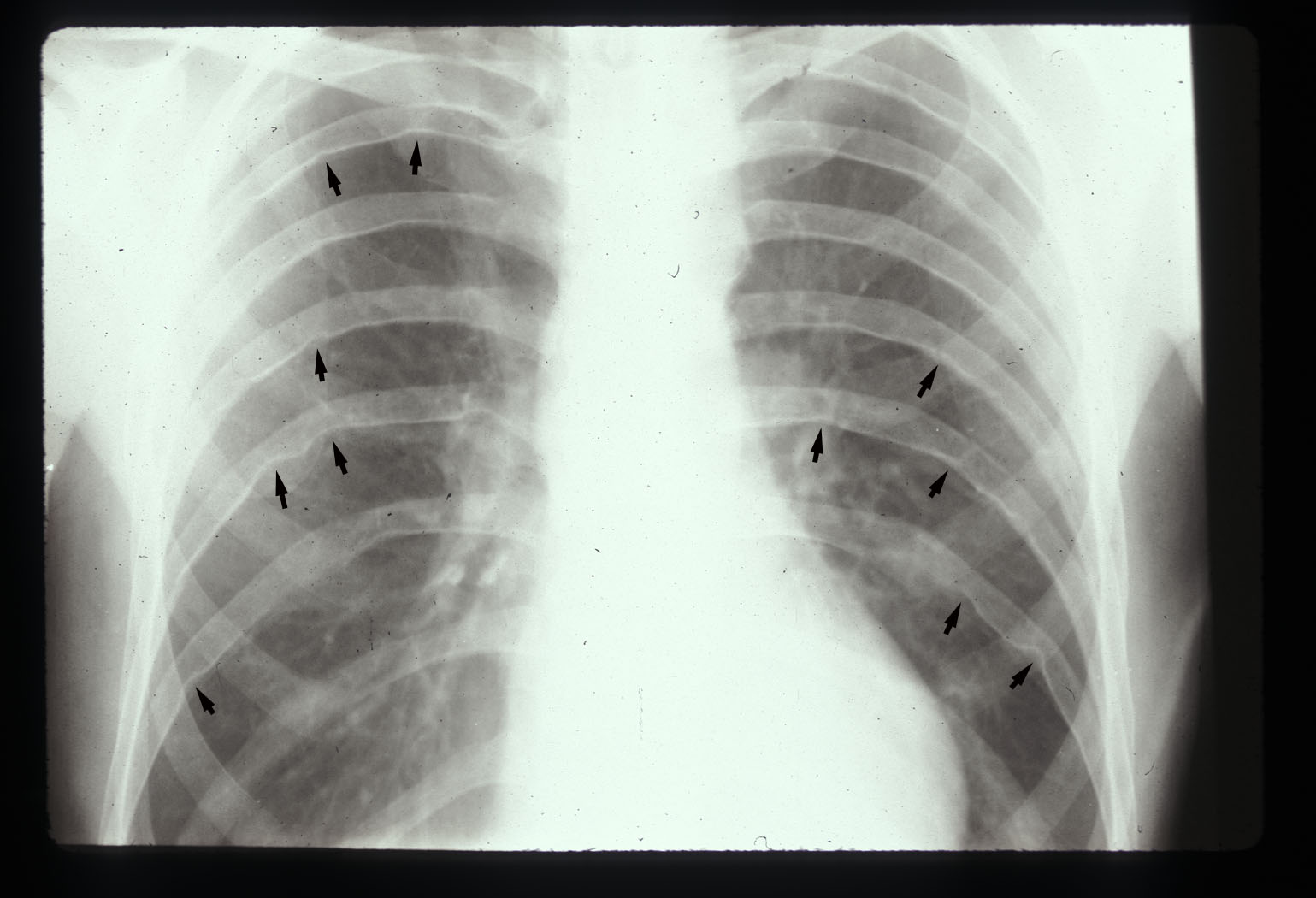
The admitting radiograph shows thin curvilinear calcification (white arrows) is seen immediately subjacent to the the lateral aspect of the aortic shadow
The distance between calcification and outer aortic edge is 4 mm.
An additional calcification (black arrow) is also found, nearly 12 mm
The previous examination (B) shows no change in thin calcifications (white arrows), but also that the larger calcification, which is now quite apart from the aortic wall, was not present at that time--indicating aortic dissection
Since atherosclerotic calcification is intimal, the distance between the calcified aortic intima, and its outer border represents the thickness of the aortic wall.
Therefore, an intimal change in this measurement, or value > 8 mm may represent changes secondary to aortic hematoma or dissection (separating the intima from rest of the aortic wall
Derived from
• Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
Question 5Posted on: Jan 13th 2019
A 72-year old woman with systemic hypertension has a chest x-ray. This radiograph shows (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Dilated pulmonary artery
- Dilated aortic arch
- Calcification of aortic arch
- Aortic aneurysm
Show Answer
Answer: Choice 3: Calcification of aortic arch indicating systemic atherosclerosis
Explanation:
The aortic arch is conspicuous but not dilated. However, notice the circumferential arch calcification (arrow heads)
The superior vena caval shadow (arrow 1) is sharp
Arrow 2 notes an incidental bony structure finding in this patient
The uppermost left contour of the cardiothoracic silhouette is the aortic arch segment
Anatomically this position of the border is formed by compression of the distal aortic arch and proximal descending thoracic aorta into a two-dimensional 'aortic knob'
The aortic arch displaces the midline trachea. Therefore, by definition, a left-sided aortic arch will displace the trachea towards the right
The contour of the aortic arch segment should be sharp
Expected normal caliber of the aortic arch should be ≤ 25 mm, measured from the left border of the tracheal air shadow to the the lateral border of the aorta
Patient rotation has a significant effect on apparent size and must be kept in mind before suggesting a pathologic diagnosis
Derived from:
• Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
Question 6Posted on: Jan 12th 2019
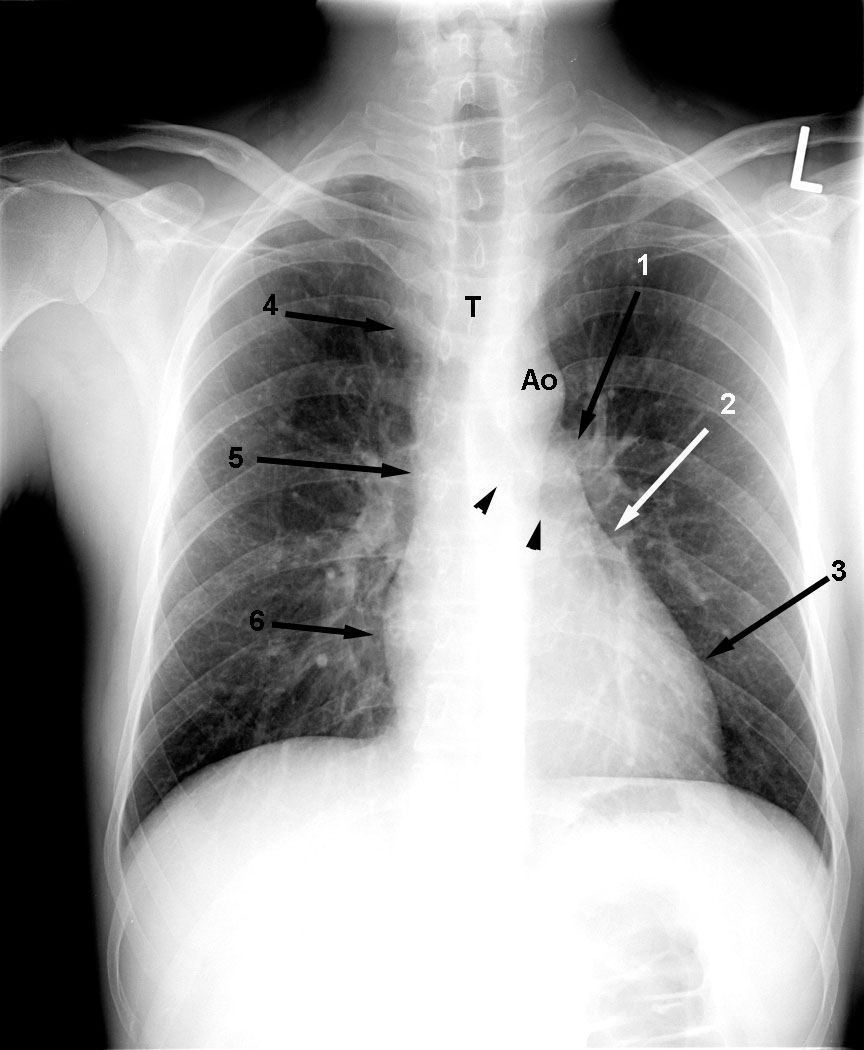
A 36-year old man has a chest x-ray (posteroanterior view). This X-ray shows (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Normal Chest-X ray
- Right sided aortic arch
- Hypertension
- Aortic aneurysm
- Pulmonary Hypertension
Show Answer
Answer: Choice 1: Normal PA examination
Explanation:
The left heart border is formed from the aortic arch segment, the pulmonary artery segment, the left atrial appendage segment and the left ventricular contour.
The left sided aortic arch (Ao) displaces the tracheal air shadow (T) towards the right
The main PA segment (arrow 1) passes just superior to the left main bronchus (black arrowheads) and is the same caliber as the Ao
The left atrial appendage segment (arrow 2) is concave towards the right.
The left ventricular contour (arrow 3) drops gently to the diaphragm.
The right cardiothoracic border is composed of superior vena cava segment, the ascending aortic segment and the right atrial segment.
The superior vena cava segment (arrow 4) lies to the right of the T
The ascending aortic segment (arrow 5) is normal, but barely makes it to the right hilum
The normal right atrial contour (arrow 6) does not extend to the descending right pulmonary artery
A useful approach is to chest x-ray is to start with area of least interest . A useful mnemonic is ATML (Are there many lesions?) where
A = Abdomen ( upper abdomen including stomach air bubble, gas in splenic flexure of the colon, the normal liver is always visible, left diaphragm and right diaphragm). Upper abdominal conditions (perforated viscus, subphrenic abscess, pancreatitis, and cholecystitis) may mimic lung disease clinically. Similarly, basilar lung disease (pleurisy, pneumonia) may mimic upper abdominal conditions .
T = Thoracic cage (soft tissue and bones including ribs, clavicle & spine)
M = Mediastinum (including heart, aortic knob, descending aorta, trachea, carina, hilum)
L = Lungs (compare left lung with right lung); look at apical, upper, mid, and lower zones & costophrenic angles
Always look at lateral views and previous chest x-rays
Derived from:
° Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
Question 7Posted on: Jan 12th 2019
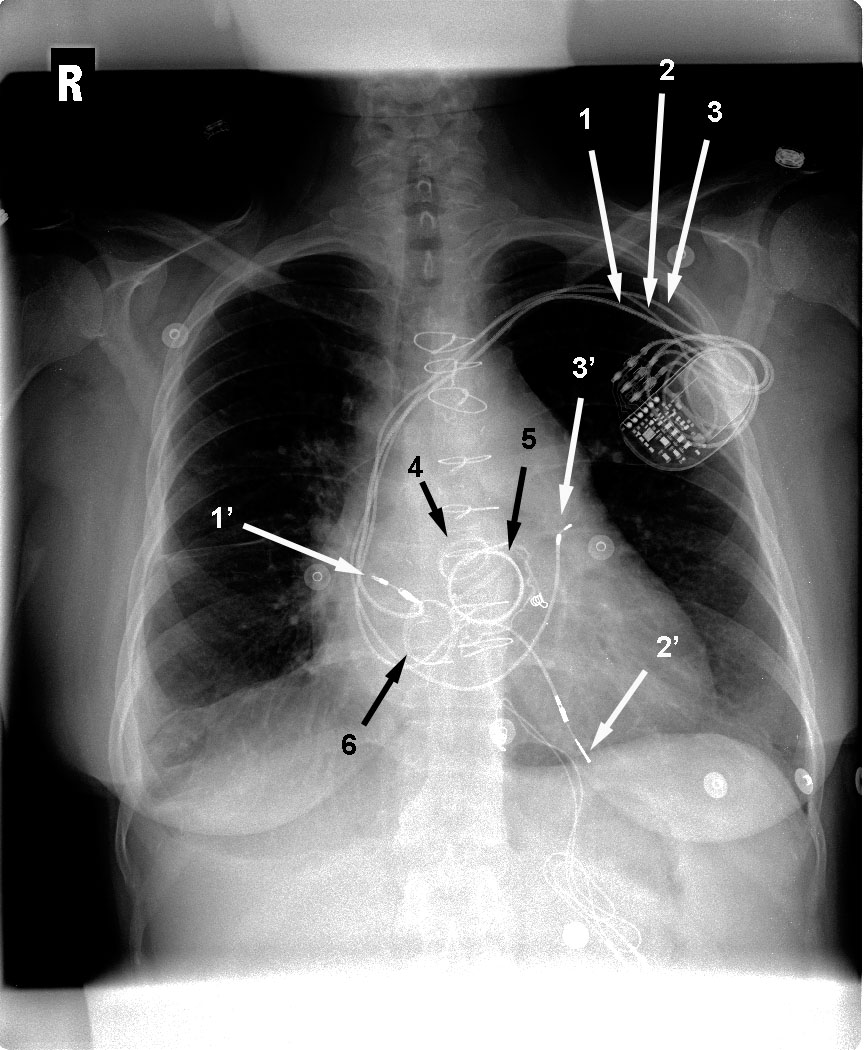
A 67-year old woman has undergone sternotomy and she has a chest x-ray. The arrow 4 is pointing towards the ring of which valve prosthesis (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Mitral Valve
- Aortic Valve
- Tricuspid Valve
- Pulmonary Valve
Show Answer
Answer: Choice 2: Aortic Valve
Explanation:
On a posteroanterior (PA) chest radiograph a reference line can be drawn from the left atrial appendages to the right cardiophrenic recess.
The aortic valve typically lies above this reference point and has the orifice oriented towards the left ventricular outlet/aortic root.
Whereas the mitral valve is below this reference line with the orifice directed towards the left ventricle/cardiac apex.
This reference line although useful in PA films, it is not useful in supine anteroposterior (AP) chest-x rays done in critically ill patients (Critical Care and Resuscitation 2006; 8: 15-18)
Typically the normal Mitral Valve Area (4.0-6.0 cm2) is greater than the normal Aortic valve area (3.0 to 4.0 cm2) and therefore replacement mitral valve ring is usually greater than aortic valve ring when both are present
Derived from:
° Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
° David J Mehlman. A pictorial and radiographic guide for identification of prosthetic heart valve devices. Prog Cardiovasc Dis. 1988 May-Jun;30(6):441-64.
Question 8Posted on: Jan 12th 2019
67-year old woman with a pacemaker has a chest x-ray. The arrow 3' shows that the pacemaker lead is in the (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
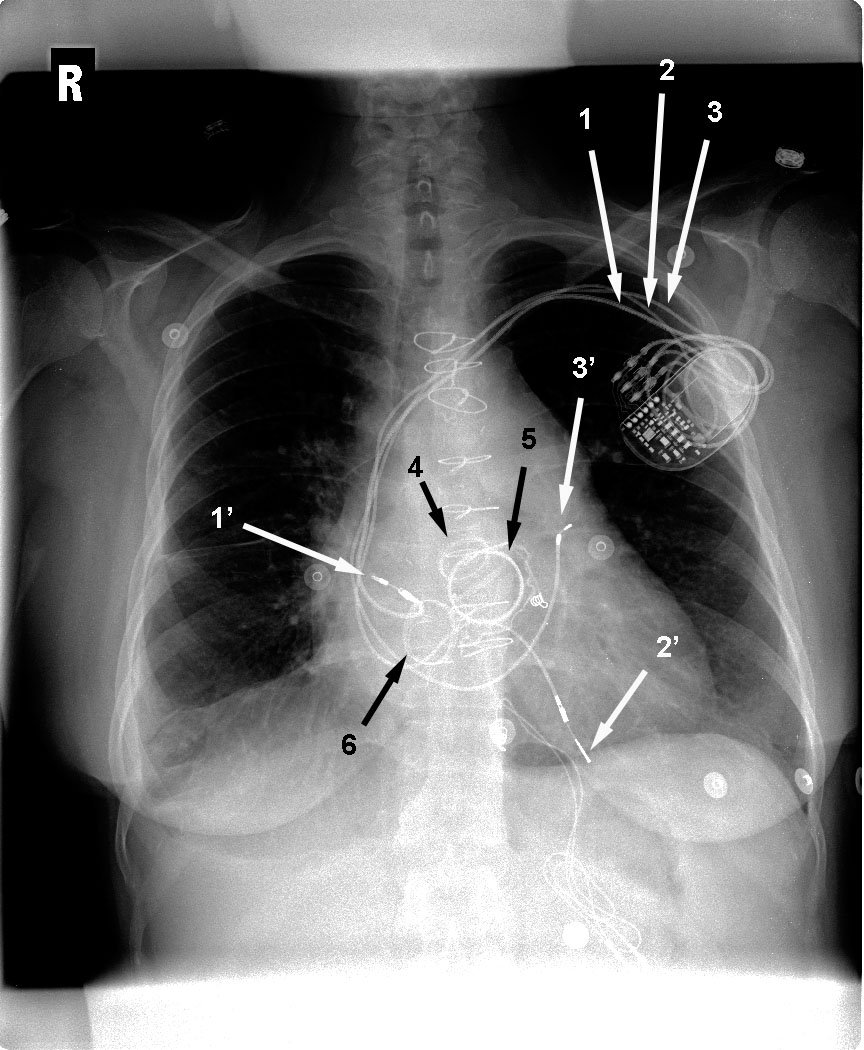
- Right Atrium
- Right Ventricle
- Coronary Sinus
- Left Pulmonary Artery
Show Answer
Answer: Choice 3: Coronary Sinus
Explanation:
This lead, directed inferiorly through the right atrium, takes a serpentine course via the coronary sinus with the tip in a posterolateral epicardial vein of the LV wall
Derived from:
° Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
° Stephanie C Torres-Ayala, Guido Santacana-Laffitte, and José Maldonado. Radiography of Cardiac Conduction Devices: A Pictorial Review of Pacemakers and Implantable Cardioverter Defibrillators. J Clin Imaging Sci. 2014; 4: 74.
° Amanda L. Aguilera, Yulia V. Volokhina , Kendra L. Fisher. Radiography of Cardiac Conduction Devices: A Comprehensive Review. https://pubs.rsna.org/doi/full/10.1148/rg.316115529
° Colleen M. Costelloe, William A. Murphy, Jr., Gregory W. Gladish and Marc A. Rozner. Radiography of Pacemakers and Implantable Cardioverter Defibrillators. American Journal of Roentgenology. 2012;199: 1252-1258 Read More: https://www.ajronline.org/doi/10.2214/AJR.12.8641
Question 9Posted on: Jan 12th 2019
This is a Chest X-Ray of a 67-year old woman. The arrow 1' shows that the pacemaker lead is in the (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
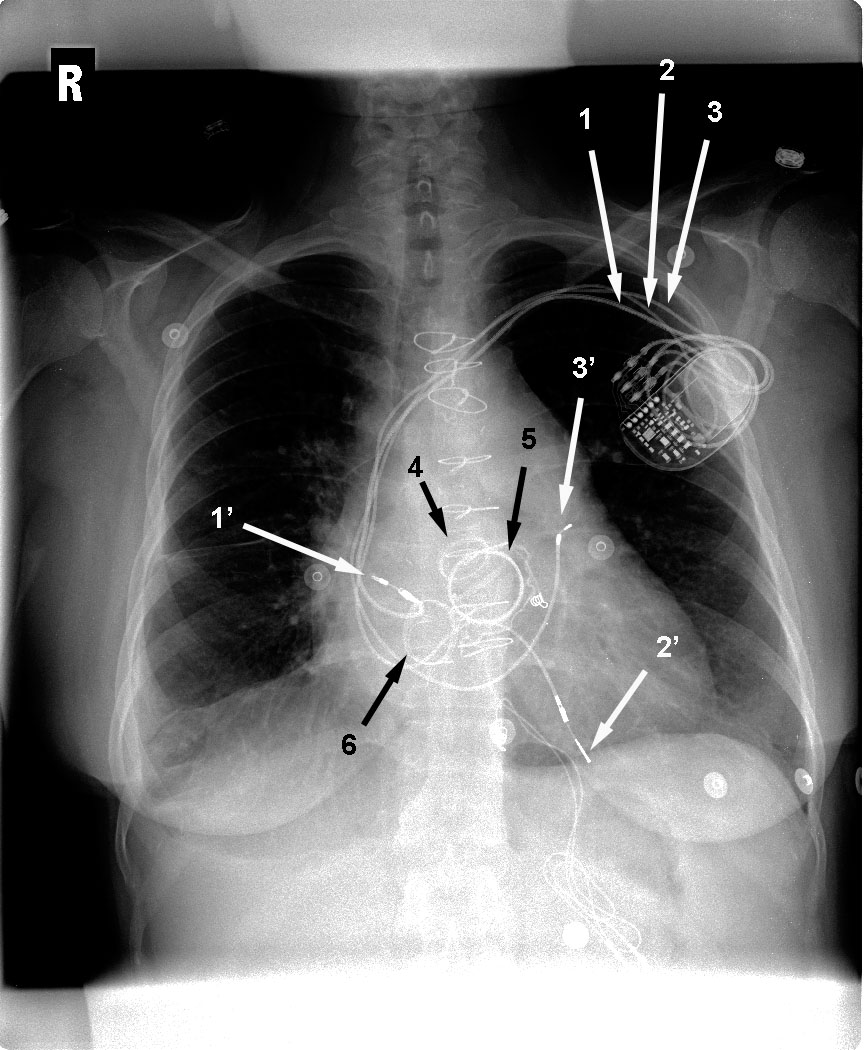
- Right Atrial appendage
- Left Atrium
- Coronary Sinus
- Right Ventricle
Show Answer
Answer: Choice 1: Right Atrial appendage
Explanation:
This lead is an inferiorly directed lead into the right atrium, which then curves anteriorly, known as the “J loop,” with the tip at the right atrial appendage
Derived from:
° Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
° Stephanie C Torres-Ayala, Guido Santacana-Laffitte, and José Maldonado. Radiography of Cardiac Conduction Devices: A Pictorial Review of Pacemakers and Implantable Cardioverter Defibrillators. J Clin Imaging Sci. 2014; 4: 74.
Question 10Posted on: Jan 12th 2019
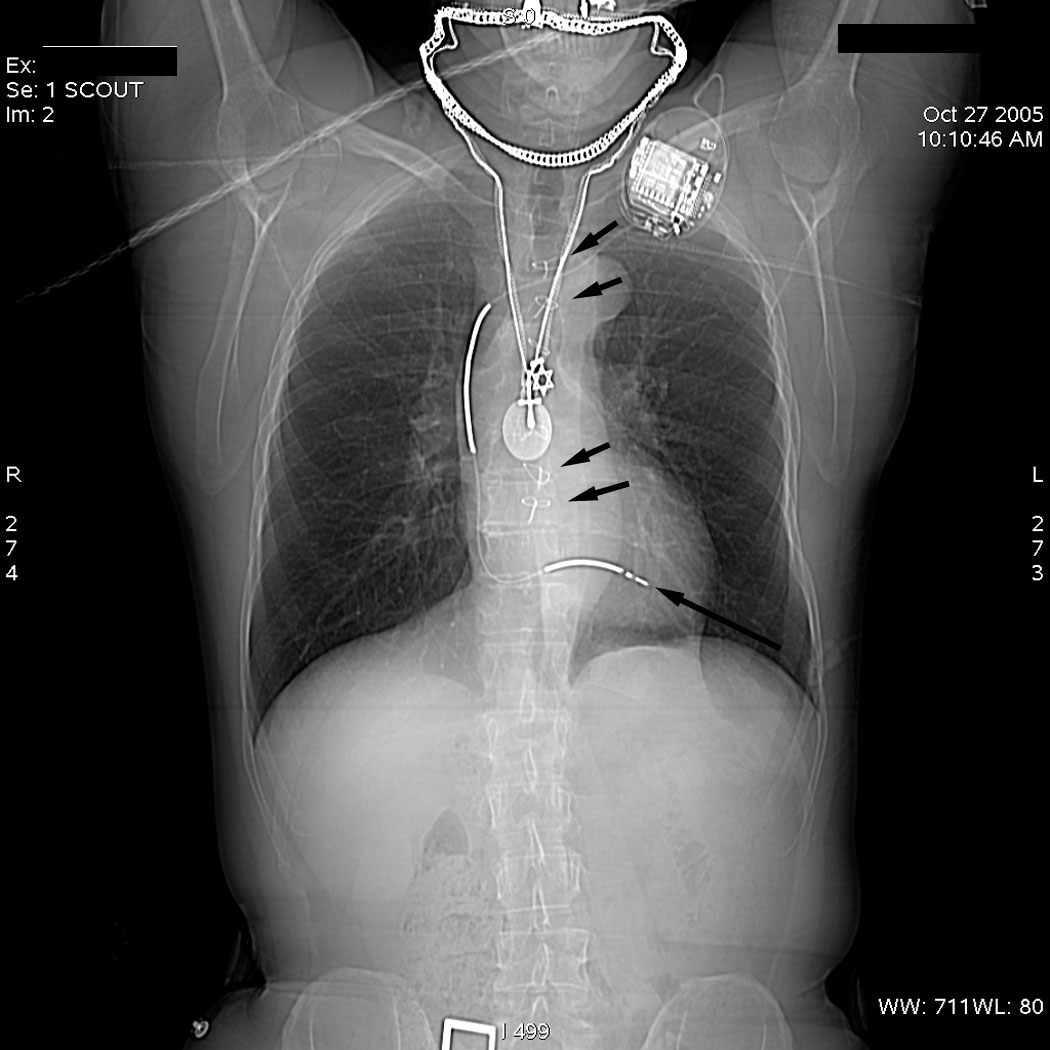
A 56-year old man complains of palpitations. His internist does a Chest X-Ray. The long arrow in this X-ray shows pacemaker lead in the (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Right atrial appendage
- Right Ventricle
- Left Ventricle
- Left atrium
Show Answer
Answer: Choice 2: Right Ventricle
Explanation:
When reading a chest x-ray identify all catheters, lines and cannulas and be sure to identify where they enter the chest and where the tips lie
Identify any extra anatomic devices or objects such as sternal sutures, ventricular assist devices, pacemakers or automated defibrillators
The RV lead is directed inferiorly through the right atrium, curves through the tricuspid valve, and ends in an anterior–inferior position at the RV apex, and is seen left of the spine on PA X-ray.
The single lead ICD has two shock coils, which are capable of generating a large amount of electrical energy in a single output to defibrillate the heart. The shock coils appear as thick bands along the course of the lead.
In this x-ray the shock coils of an ICD lead appear as sections of thickened metallic opacity that terminate in the regions of the superior vena cava and right ventricle.
Derived from:
° Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
° Stephanie C Torres-Ayala, Guido Santacana-Laffitte, and José Maldonado. Radiography of Cardiac Conduction Devices: A Pictorial Review of Pacemakers and Implantable Cardioverter Defibrillators. J Clin Imaging Sci. 2014; 4: 74. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4286824/
Question 11Posted on: Jan 12th 2019
A 52-year old male has hypertension. The distal pulses in his legs are not well felt. This Chest X-ray shows (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Prominent aortic arch
- Rib notching
- Cardiomegaly
- Lung Cancer
Show Answer
Answer: Choice 2: Rib-notching
Explanation:
The aortic arch segment is small
There are multiple erosions along the undersides of the upper and mid ribs (short arrows)
Rib notching is a consequence of dilated intercostals collateral blood flow in coarctation of aorta
It is rarely seen in individuals below the age of 8 or 9 years
Rib notching, when present, typically has a wavy, lucent (eroded) appearance along the underside of mid-to-upper ribs, immediately subjacent to a sclerotic, proliferative bony response to the pulsating systolic expansion against bone
Derived from: Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
Question 12Posted on: Jan 12th 2019
A 60-year old complains of shortness of breath. Her internist orders a Chest X-ray. This Chest X-ray shows (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)"
- Enlarged heart
- Pectus excavatum
- Rib notching
- Sternal sutures
Show Answer
Answer: Choice 2: Pectus excavatum
Explanation:
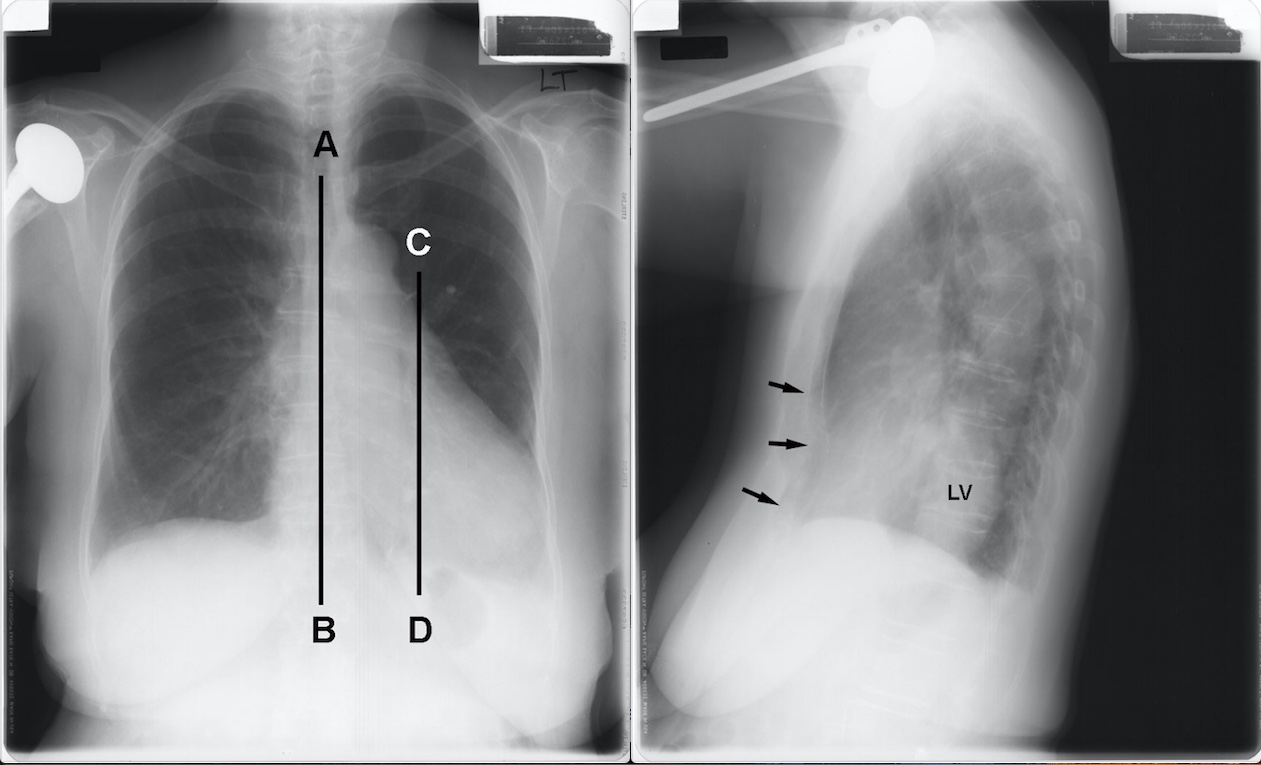
The PA x-ray shows displacement of the heart to the left. Line CD is drawn through the mid portion of the heart. Notice the heart is displace to the left of the midline AB
The lateral view shows indentation of the sternum (arrows) and pushes the heart. The left ventricle (LV) is projected over the lower thoracic spine
A normal heart may look abnormal because of rotation or displacement within the chest secondary to pectus deformity, scoliosis of kyphosis
Particularly in patients with pectus deformity the anterioposterior dimension of the chest is decreased resulting in the heart being displaced to the left ---giving the impression of clockwise rotation and right heart enlargement (as shown in this image)
Derived from: Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR (Editor). Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516
Question 13Posted on: Jan 8th 2019
A 34-year old with previous history of a sternotomy, complains of shortness of breath. This chest X-Ray shows (Courtesy Amgad N. Makaryus, MD Chairman of Cardiology, Nassau University Medical Center, NY & Lawrence M. Boxt, MD Englewood Hospital Medical Center, NJ)
- Normal Chest-X Ray
- Absent Aortic Arch
- Asymmetry of the left upper rib
- Choices 2 & 3
Show Answer
Answer: Choice 4: Absent aortic Arch and Asymmetry of the Left Upper Rib
Explanation:
In this chest x-ray the trachea is in the midline and there is no apparent aortic arch segment
Notice (arrow) the asymmetry of the left upper rib, secondary to previous surgery to repair an aortic arch coarctation
Fractures and asymmetric interspaces may be the only information relating to earlier palliative or curative cardiothoracic surgery
In evaluating a chest x-ray it important to have a routine in assessing it beginning with the osseous structures--look at all the ribs and interspaces between them
Makaryus AN, Boxt LM. Chest Radiography: What the Cardiologist Needs to Know in Baliga RR. Cardiology: McGraw Hill Specialty Board Review. 2012, pg 499-516